 Hannah Ostrem
Hannah Ostrem
National Nurses Day: Celebrating Nurses Everywhere
National Nurses Week kicks off today with National Nurses Day, an important time to acknowledge and appreciate the people who stand at the center of...

UPDATED April 21, 2021: This article has been revised, updated, and expanded for current accuracy and comprehensiveness.
IT'S A FACT: Your patients are having Large Vessel Occlusion (LVO) strokes, whether your facility has protocols in place to manage them or not. So what exactly is an LVO stroke and what's your plan for treating these patients?
If you don't have a plan that works EVERY SINGLE TIME, then you are falling below the national standard of care.
Large Vessel Occlusion (LVO) strokes are a type of ischemic stroke and occur when a major artery in the brain is blocked. An LVO stroke blockage occurs in one of the following major cerebral vessels in the brain:
In contrast, a small vessel occlusion is an occlusion of one of the smaller cerebral vessels in the brain that are unable to be cannulated by mechanical thrombectomy and are better treated with IV thrombolysis. LVO strokes are considered one of the more severe kinds of strokes, accounting for approximately 24% to 46% of acute ischemic strokes. For this reason, acute LVO stroke patients often need to be transported to more comprehensive centers equipped to handle LVOs.
The signs and symptoms of a stroke can be vague to many people—their main complaint often being something like, "I feel off today." Because of this, many patients delay getting medical attention, opting instead to rest or nap. Stroke symptoms include things like the sudden loss of balance or coordination, blurred vision, face drooping, weakness in one arm, and slurred speech. But these "vague symptoms" are extremely serious. This is why it's so important to immediately call emergency services at the first signs of a possible stroke. From there, paramedics will assess the patient and transport them to the hospital. (And by using mobile communication technology like Pulsara to improve stroke care, clinical teams can reduce door to needle times to achieve the best possible patient outcomes for acute stroke patients.)
(Check out "Large Vessel Occlusion Strokes: How To Assess LVO Patients" to learn more)
LVO stroke symptoms can mimic normal stroke symptoms. For that reason, the BE FAST acronym can be one of the best guides to help evaluate a patient for LVO stroke symptoms. (Other scales created to help identify stroke—that you should add to your base knowledge of care—include the Cincinnati Prehospital Stroke Scale, Los Angeles Motor Score, NIH Stroke Scale, and Rapid Arterial Occlusion Evaluation.)
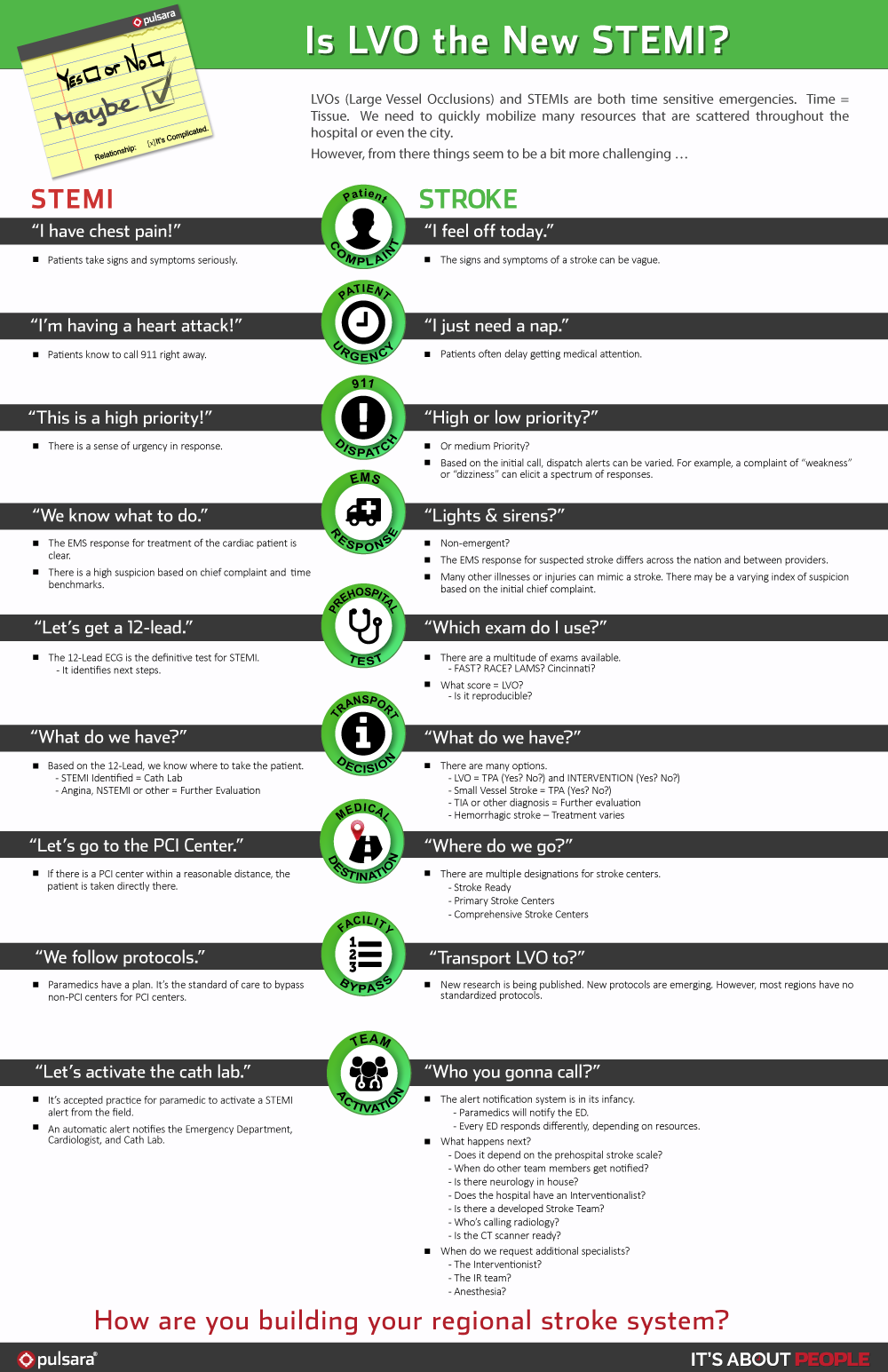
LVO is NOT, in fact, the "STEMI of the stroke world." It is far more complex, it is not binary, and it requires the utilization of different resources at different points in time.
As you'll see in the infographic below, managing your LVO patients just like you manage STEMI patients is probably not the best approach. LVOs and STEMIs are both time-sensitive emergencies. (Time = Tissue!) We need to quickly mobilize many resources that are scattered throughout the hospital or even the city. However, from there, things are a bit more challenging...
Check out the infographic below to understand the breakdown.
Download PDF of Infographic | Download Image Infographic
![]()
Click here to learn how CHRISTUS Good Shepherd Health System achieved a 59% Decrease in average door-to-needle time for stroke patients receiving tPA with Pulsara.

National Nurses Week kicks off today with National Nurses Day, an important time to acknowledge and appreciate the people who stand at the center of...

Over the past decade, a growing body of research is establishing a powerful consensus: cross-functional, real-time care team communication is a...

In just a few days, one of the world’s largest mass gatherings is taking place—all while we’re asleep. With millions of bunnies descending on...