 Tim Hakamaki
Tim Hakamaki

Pulsara Around the World - March 2026
February Recap From neuroscience symposiums to EMS expos, our teams traveled to five shows in February. Our events schedule is slowing down in March....
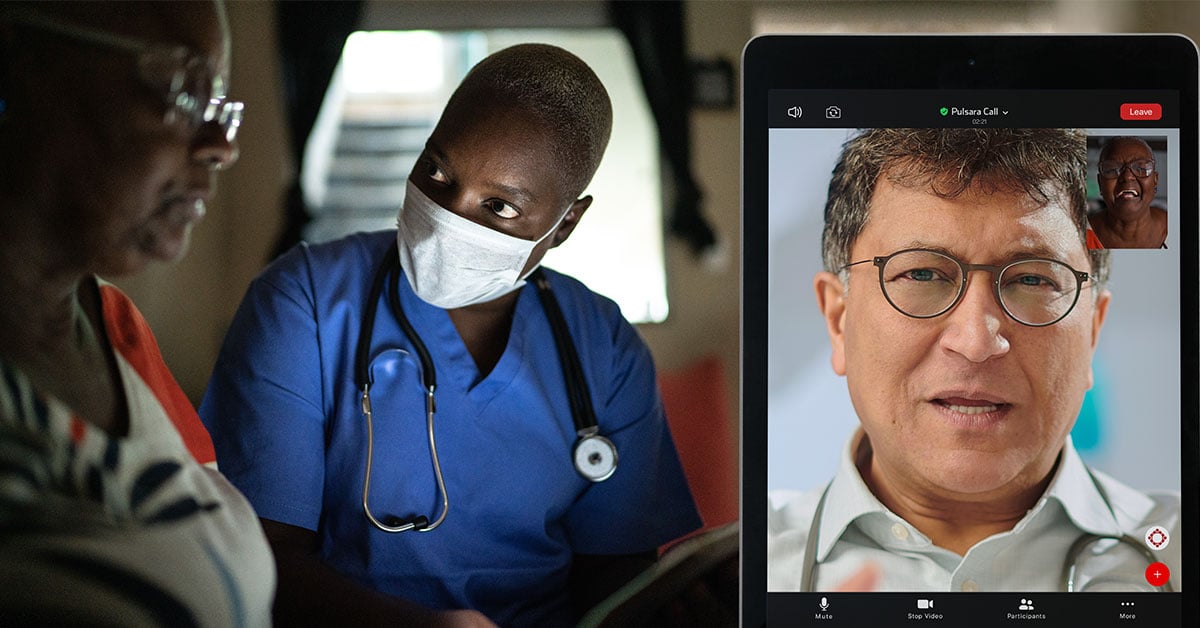
![Finding a Next-Generation Telehealth Plan of Action for Your Hospital [Part 2]](https://www.pulsara.com/hubfs/video-chat-medic-hosp-1180x700.jpg)
This is part 2 of our 5-part blog series based on the webinar “The Next-Gen Communication and Telehealth Plan of Action for Your Hospital.” Check out part 1 here. Watch the corresponding section of the webinar below, or listen to the full webinar here.
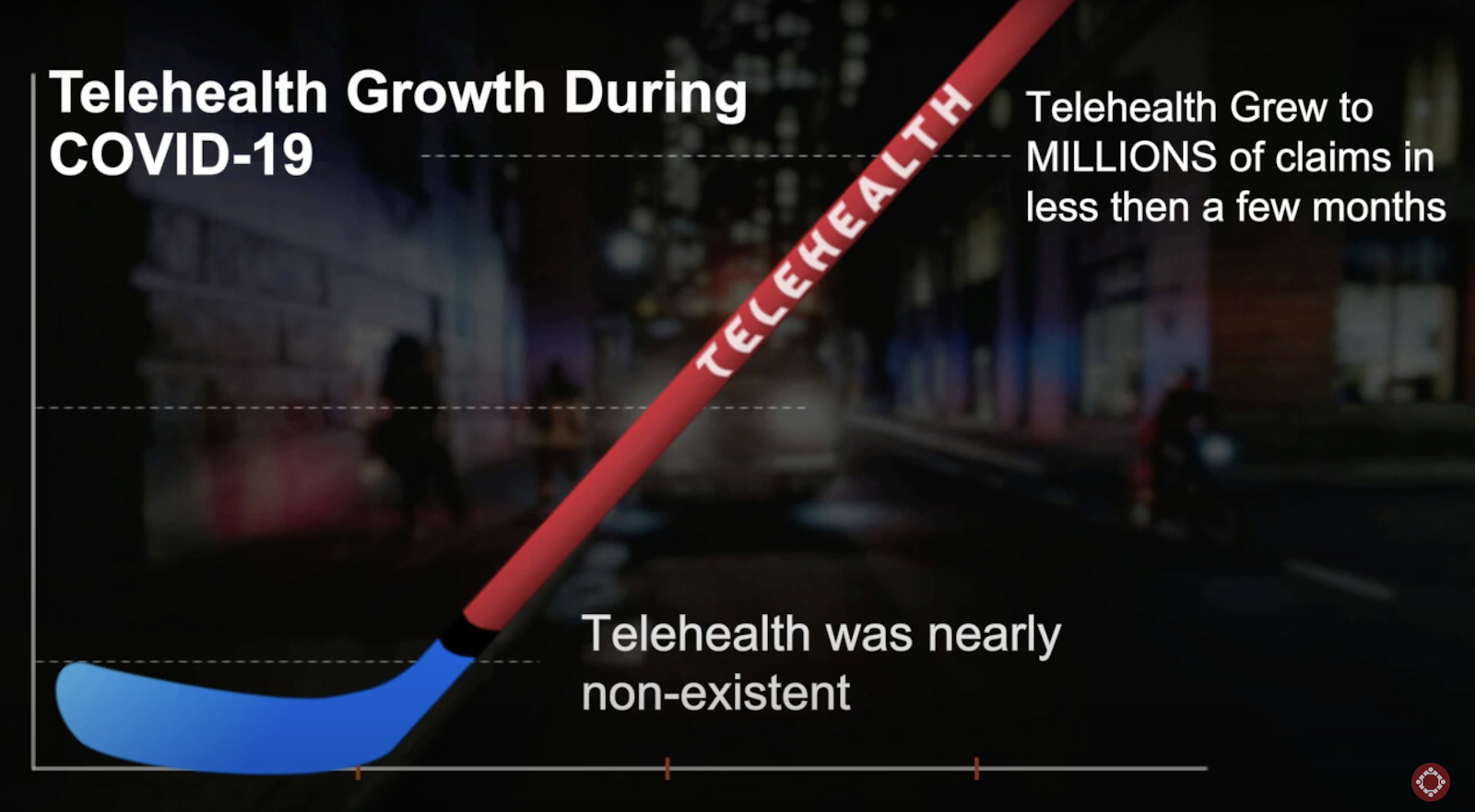
Over the last four months, COVID-19 has forever changed the landscape of healthcare. Telehealth has experienced explosive growth since March, creating groundbreaking changes in telemedicine regulations and reimbursement opportunities. Prior to four months ago, only a small minority of systems utilized telehealth in beyond three to five percent of their appointments. Since the start of COVID-19, telehealth has grown to millions of claims in less than a few months. According to a published stat, the number of Medicare beneficiaries using telehealth services during the pandemic increased 11,700%.
Looking at a graph of telehealth’s "hockey stick" growth is astonishing. For many years, there was no substantial change. March 2020 marks the shift between the blue and red growth markers. Telehealth shot from near non-existence to millions of claims practically overnight.
Such a stunning rate of growth over such a short period of time begs the question: why hasn’t telehealth expanded like this previously?
The answer is simply that policy barriers made the expansion of telehealth nearly impossible for the last 10 years. In the early days of telehealth, it was clear that there was a desperate need for telehealth services in rural areas. A shortage of available health resources and difficulty in recruiting new doctors to rural areas made telehealth an obvious opportunity for expanding health coverage. As a result, much of the policy surrounding telehealth was then written around making it available to rural areas. Unfortunately, this ended up becoming a catch-22. Policies like the originating site rule set very specific requirements around where a patient had to be located for the visit to be considered a billable encounter. Restrictions also prevented physicians from seeing patients across state lines.
Medicare telehealth coverage prior to COVID-19 required that services normally be provided in-person, and conducted by interactive audio/video with two clinicians present: one in person, one remote. One on-site caregiver needed to be present with the patient, and the other clinician, located remotely, would participate in the interaction through a monitor. This type of care was typically only available for beneficiaries in rural areas—and in most cases, beneficiaries could not stay at home. The visit had to be conducted at a local office. Not only that, caregivers could only provide evaluation and management, or mental health services. Using phones to conduct the encounter was not permitted.
Virtual check-ins, on the other hand, were not normally offered in person. These encounters were brief, paid at a very low rate, and could only be offered to established patients. As with the rest of healthcare, telehealth especially, these services could only be offered by practitioners who could utilize the appropriate Evaluation and Management HCPCS and CPT codes.
Once COVID-19 hit, everything changed. Telehealth became an efficient, easy way for physicians to continue to care for patients without needing to see them in person. As telehealth usage skyrocketed, the Centers for Medicaid and Medicare Services (CMS) and third parties reacted quickly to loosen restrictions for the pandemic. The CMS provided the following chart as a road map of some of the changes in telehealth restrictions and coding for reimbursement.
The CMS greatly extended Medicare’s coverage of telehealth and virtual check-ins. At a high level, you can see how Medicare telehealth visits have been redefined, and which related CPT and HCPCS codes have been affected. The chart also notes that certain services that were previously required to be offered only to established patients have been temporarily suspended, and will likely remain so until the crisis is over. It’s a similar story with virtual check-ins. The chart provides a road map for the CPT codes, and then adds more definition to virtual check-ins, calling them “brief,” five-to-ten minute appointments.
Beneficiaries can now receive services from their home, which is a game-changer. The strict location guidelines were long one of the major barriers to telehealth expansion. Mobile devices and phones can also now be utilized to provide these services, and audio-only calls are now covered. More practitioners are now permitted to provide speech therapy, occupational therapy, and physical therapy (ST/OT/PT) services over telehealth, expanding the reach of all of those services—and the associated HCPCS codes and CPT codes. Virtual check-ins may now be offered to new patients, and more practitioners can now bill for these services.
 At least for the duration of the pandemic, telehealth is no longer restricted to rural areas, and neither is placing specific service codes on a claim. Independently, this has been the single largest improvement for telehealth. Telehealth now has the largest global impact of other healthcare services, like home care, mobile integrated health, and other hospital services.
At least for the duration of the pandemic, telehealth is no longer restricted to rural areas, and neither is placing specific service codes on a claim. Independently, this has been the single largest improvement for telehealth. Telehealth now has the largest global impact of other healthcare services, like home care, mobile integrated health, and other hospital services.
In late June, the Equal Access to Care bill was introduced in Congress, which, if passed, would allow telehealth to be practiced anywhere for up to 180 days beyond the pandemic ending. It's also important to note that Congress and other policymakers have held feedback sessions with industry leaders to sort through which changes should remain in place after the pandemic. All the updates are being considered, but the following suspensions are receiving careful consideration: care from anywhere, which is the new lift on the rural requirement, and expanded practitioner services, which are the new CPT and HCPCS codes for ST/OT/PT. Careful thought is also being put toward how to achieve payer parity; if all payers have a different requirement, it adds an additional level of complexity.
So what does the future look like? With so many changes happening so quickly, everyone is looking into a crystal ball and trying to predict the unpredictable.
Regardless of what does happen, though, it’s clear that right now is the time to adopt telehealth solutions that allow room for flexibility and adjusting to the changes that will continue to occur. The COVID-19 pandemic is putting a strain on the healthcare system, but accurately capturing and documenting cases for the coronavirus can provide a nice blueprint and roadmap going into the future.
Recapturing volume and revenue quickly with telehealth will be critical to finding stability and resuming normal operations. Telehealth is growing a segment of accounts receivable for most organizations. As such, hospitals must utilize an analytics-driven approach to boost volume, maximize revenue, and accelerate cash. Your telehealth solution must be efficient, flexible enough to scale up or down to meet your hospital’s needs, and must integrate into the clinical workflows to maximize reimbursement. And while telehealth regulations will never go back to what they were before the pandemic, they are also not likely to remain as flexible as they are now. Your telehealth system needs to be HIPAA-compliant and specifically designed for healthcare, so that it can continue to serve you long after COVID-19 ends.
 Another thing to consider is how adopting a telehealth solution will impact—and hopefully help—your team. Though it will help streamline workflows, your team will have to get used to the new systems for scheduling, documentation, billing, referral processes, specialty care, urgent care, and emergency care services. Training staff on the policies, practices, and protocols of using telehealth can be quite a load, and can make or break the experience. Adopting an intuitive solution that can take care of all those things will make things easier and prevent more frustration than you might first realize.
Another thing to consider is how adopting a telehealth solution will impact—and hopefully help—your team. Though it will help streamline workflows, your team will have to get used to the new systems for scheduling, documentation, billing, referral processes, specialty care, urgent care, and emergency care services. Training staff on the policies, practices, and protocols of using telehealth can be quite a load, and can make or break the experience. Adopting an intuitive solution that can take care of all those things will make things easier and prevent more frustration than you might first realize.
In the coming months, we’ll learn more about what the future of telehealth will look like. If one thing is certain, though, it’s that telehealth will never return to what it was before the COVID-19 pandemic. The future of telehealth holds a great deal of potential for positive innovation. If your hospital doesn’t already have a solid solution in place, now is the time to look for one.
In part 3 of this series, Pulsara’s Founder and CEO, Dr. James Woodson, will take an in-depth look at the expanding communication capabilities of telehealth services, and how they can replace the many interoperable communication technologies currently used in healthcare.
![]()
To learn more about creating a next-generation communication and telehealth plan for your hospital, listen to the full webinar here.

February Recap From neuroscience symposiums to EMS expos, our teams traveled to five shows in February. Our events schedule is slowing down in March....

January Recap The start of 2026 was on the slow side for our events schedule, with our team heading to the Florida Fire & EMS Conference, the...
Recent research shows how Pulsara was successfully leveraged to connect more than 6,000 COVID-19 patients to monoclonal antibody infusion centers via...